
Surgical repair of the congenital malformation, i.e., ureteropelvic junction obstruction can be performed by the transperitoneal or retroperitoneal approach. The choice of the approach depends on the preferences of the operating surgeon. In our Department, the transperitoneal approach is most frequently selected with the use of 3 or 4 trocars: 1 x 5 mm and 2 x 10 mm (optionally 2 x 5 mm and 1 x 10 mm). The optical system is 10mm and the inclination angle is 30°. Optionally, the 5mm or even 3mm optical system is used and 3mm instruments (mini-lap). Procedures with the use of 5mm or 3 mm instruments are technically difficult, yet preferred in young and slim patients. The number of instruments used depends on the Department’s equipment and the operating surgeon’s preferences.
POSITIONING THE PATIENT
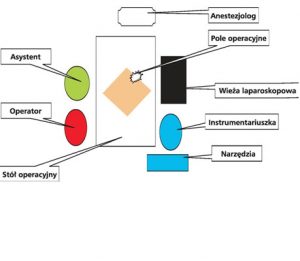

The patient is lying on the back with the operated side elevated. The operating surgeon and assistant stand side by side, on the side opposite to the operated one. The laparoscopic tower with the monitor stands on the side of the operated kidney, opposite the operator and the assistant.
The procedure begins with an incision of the skin under the umbilicus, insertion of the Veres needle and insufflation of the peritoneal cavity. Then, in the same place, the first trocar (optics) is inserted. Under visual control, other trocars are inserted for the operator’s and assistant’s instruments: in the epigastrium, midway between the sternal xiphoid process and the umbilicus, in the mid-abdomen and in the midclavicular line. The fourth additional trocar is placed (if need arises) in the epigastrium in the midclavicular line.
THE COURSE OF THE PROCEDURE
Stage I – visualisation of the retroperitoneal space.
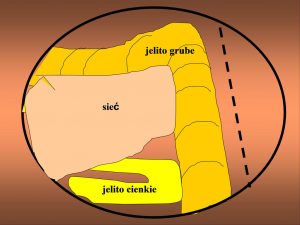
After inserting the optical system, the peritoneal cavity is inspected. The large intestine, hepatic or splenic flexure – depending on the operated side – are visualised. The patient is placed on the back, with the operated side slightly elevated. The peritoneum is incised above the large intestine which is moved back to the hepatic or splenic flexure, depending on which side is operated on. After shifting the intestines, the retroperitoneal space is exposed and the iliopsoas muscle is visualised. This muscle is the key point of reference in laparoscopic surgery.
Stage II – dissection of the renal pelvis
Moving along the iliopsoas muscle, the ureter is dissected just below the ureteropelvic junction. Moving upwards along the ureter, the renal pelvis is reached. After separating the renal pelvis from the surrounding tissues, the strictured section of the ureteropelvic junction is cut off.
Stage III – cutting off the ureteropelvic junction
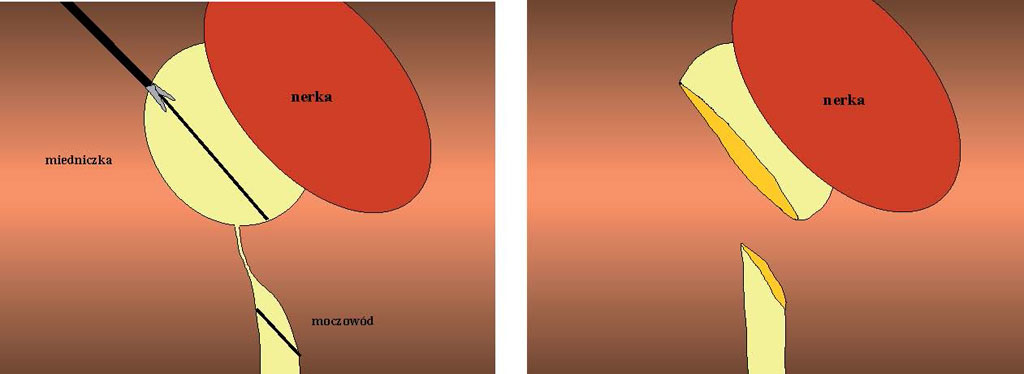
The renal pelvis along the transverse axis is incised and the ureter below the strictured section connecting it with the pelvis is cut off. The ureter is incised on a section of approx. 1.5 cm long.
Stage IV – anastomosis of the renal pelvis and the ureter
The needle is inserted by the trocar. A typical 3-0 Vicryl suture or a V-loc suture can be used. The first suture is placed on the ureter starting from the outside to the inside and on the renal pelvis from the inside to the outside. The suture is not cut off. The needle and suture are placed under the ureter. A continuous suture is placed on the posterior wall of the renal pelvis, and further inside the pelvis. At this stage of the procedure, a Double-J catheter can be inserted into the ureter. Next, a second continuous suture is placed on the anterior wall of the renal pelvis, thus connecting it with the previously incised ureter. This suture is then extended to the renal pelvis. A Redon drain is left in the retroperitoneal space.
ORIGINAL BYDGOSZCZ TECHNIQUE
Throughout two decades of experience, we have introduced our own original modifications of certain procedures. The Bydgoszcz-origin modification of surgical repair of ureteropelvic junction obstruction presents as follows: after separating the renal pelvis from the surrounding tissues, the first incision is made. The pelvis is incised along the transverse axis, and the incision is directed towards the ureter. The ureteropelvic junction is incised and extended approx. 1.5 to 2 cm on the anterior wall of the ureter. At this stage of the procedure, the ureteropelvic junction is not completely severed. The needle is inserted, and the V-loc suture is used. The first suture is placed on the ureter, starting from the outside to the inside and on the pelvis from the inside to the outside. The sutures are knotted, yet not cut off. The needle and suture are placed under the ureter. It is only at this stage that the excess of the renal pelvis together with a fragment of the ureter and the ureteropelvic junction is cut off. A continuous suture is placed on the posterior wall of the renal pelvis, and further inside the pelvis. After suturing the posterior wall, the suture is cut off. At this stage of the procedure, a Double-J catheter can be inserted into the ureter. Next, a second continuous suture is placed on the anterior wall of the pelvis, thus connecting it with the previously incised ureter. This suture is then extended to the pelvis. A Redon drain is left in the peritoneal cavity.