

Laparoscopic nephrectomy can be performed by transperitoneal (laparoscopic nephrectomy) in the supine position or retroperitoneal approach (retroperitoneoscopic nephrectomy) in the lateral position. The choice of the approach is at the surgeon’s discretion and depends on the operator’s preferences. In our Department, laparoscopic (transperitoneal) approaches are used to remove a kidney due to cancer or hydronephrosis. The retroperitoneoscopic (retroperitoneal) approach is applied to remove small cirrhotic kidneys.
LAPAROSCOPIC NEPHRECTOMY (TRANSPERITONEAL APPROACH)
Transperitoneal approach is used for removal of kidney tumours and large hydronephrosis because it offers more space, which facilitates the removal of large organs (cancer, hydronephrosis). There is more surgical freedom of movement. The instruments can be placed at such a distance so as to avoid any collision, which is often the case in this approach.
The kidney removal procedure is performed with the use of 3 or 4 trocars: 2 x 5 mm and 2 x 10 mm (optionally 2 x 5 mm and 1 x 10 mm and 1 x 12 mm). The optical system is 10mm and the inclination angle is 30°. The number and type of instruments used depends on the operator’s preferences.
POSITIONING THE PATIENT

The patient is lying on the back with the operated side elevated. The operator and assistant stand side by side, on the side opposite to the operated one. The laparoscopic tower with the monitor is placed on the side of the operated kidney, opposite the operator and the assistant.
The procedure begins with an incision of the skin under the umbilicus, followed by insertion of the Veres needle and insufflation of the peritoneal cavity. Then, in the same place, the first 10 mm trocar (optics) is inserted.


Under visual control, other trocars are inserted for the operator’s and assistant’s instruments: in the epigastrium, midway between the sternal xiphoid process and the umbilicus, in the mid-abdomen and in the midclavicular line. The fourth additional trocar is placed in the epigastrium in the midclavicular line.
THE COURSE OF THE PROCEDURE
Stage I – visualisation of the retroperitoneal space
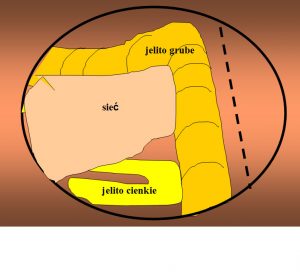
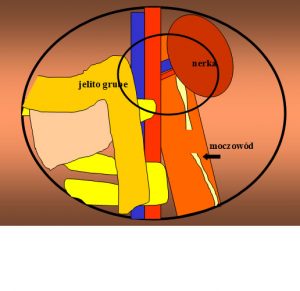
After inserting the optical system, the peritoneal cavity is inspected. The large intestine, hepatic or splenic flexure – depending on the operated side – are visualised. The patient is placed on the back, with the operated side slightly elevated, therefore the intestines are slightly going down. The peritoneum is incised above the large intestine which is moved back to the hepatic or splenic flexure, depending on which side is operated on. After shifting the intestines, the retroperitoneal space is exposed and the iliopsoas muscle is visualised. This muscle is the key point of reference in laparoscopic surgery.
Stage II – visualisation of the renal hilum
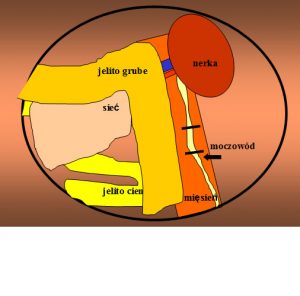
Under visual control, other trocars are inserted for the operator’s and assistant’s instruments: in the epigastrium, midway between the sternal xiphoid process and the umbilicus, in the mid-abdomen and in the midclavicular line. The fourth additional trocar is placed in the epigastrium in the midclavicular line.
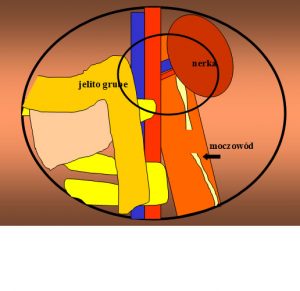
Stage III – dissection and cutting renal vessels
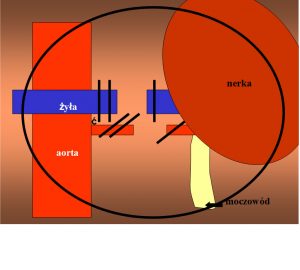
At this most important stage of the procedure, the renal vessels are dissected. In laparoscopy, the zoom function enables a significant magnification of the image and acute visualisation of the kidney pedicle. In the traditional approach, the vein is in front and covers the artery.
The optical system with the inclination angle of 30 ° when rotated allows to look under the vein and dissect the artery first. We want to close the artery first, and then the vein. This is, of course, the most difficult stage of the procedure and it requires precision and composure. After the pedicle is dissected, 2 or 3 special plastic clips are placed on the renal artery. The renal vein is usually wider, therefore in order to close it, we use special 15 mm long clips inserted through a 12 mm trocar or an even longer automatic vascular endostapler. After closure, the vessels are cut between the clips.
Stage IV – cutting off the renal poles
After closing the vessels, the kidney is to be released from the surrounding tissues. The kidney with the renal adipose capsule is cut off from the base with scissors. Its inferior pole and posterior margin are visualised by pulling upwards the dissected ureter. This stage of the procedure is not difficult. Releasing the superior pole is more complicated. Usually the assistant’s help is needed to lift the liver, using the retractor, on the right or the spleen on the left. Damaging these organs in laparoscopy is rare due to good visualisation of the surgical site.
If it is necessary to remove the adrenal gland, dissection and clipping or coagulation of small vessels arising from the aorta and inferior vena cava and from the diaphragm is necessary. If we do not remove the adrenal gland, then we cut it off from the kidney using a harmonic knife or dissector with bipolar coagulation, or scissors with monopolar coagulation.
Stage V – extraction of the kidney
The kidney, together with the renal adipose capsule, is placed in a special bag. At this stage of the procedure, the surgical bed after the removed organ is inspected, hemostasis of small vessels is carried our and a drain is inserted. Then the organ placed in the bag is extracted. This can be done by making a small 4 cm-long incision, e.g. in the hypogastrium. We can also morcellate the kidney inside the bag using forceps or a morcellator, and then extract it outside through a 10 mm trocar.
At the end of the procedure, the places remaining after the insertion of 10-12 mm trocars are dressed by suturing fascias and the skin. Only skin sutures are applied on places remaining after the insertion of 5 mm trocars.
RETROPERITONEOSCOPIC NEPHRECTOMY (RETROPERITONEAL APPROACH)


Retroperitoneal approach is better in certain cases than conventional laparoscopy.
The procedure does not affect the peritoneum, and in the peritoneal space there are no organs that are most often accidentally damaged during laparoscopy, i.e. intestines, liver, or spleen.
In the retroperitoneal space, after inserting the trocars, the ureter and the kidney are directly in front of the optical system. The disadvantages of retroperitoneal approach are the need to perform the procedure in a small confined space, close proximity of trocars and instruments, and the lack of points of reference.
The retroperitoneoscopic nephrectomy is performed with the use of 3 or 4 trocars: 1 – 2 x 5 mm and 2 x 10 mm (optionally 1 – 2 x 5 mm, 1 x 10 mm and 1 x 12 mm). The optical system is 10mm and the inclination angle is 0° or 30°. The number and type of instruments used depends on the operator’s preferences.
POSITIONING THE PATIENT
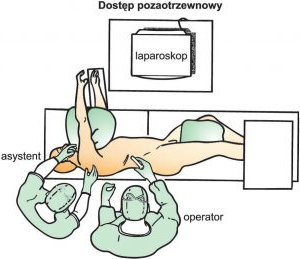
The patient is lying on the back as in the traditional Bergman-Israel incision, i.e. the same as during the conventional removal of the cirrhotic kidney.
The operator and the assistant stand side by side, on the side of the operated kidney. The laparoscopic tower with the monitor stands on the side opposite to the operated one.
INSERTING TROCARS
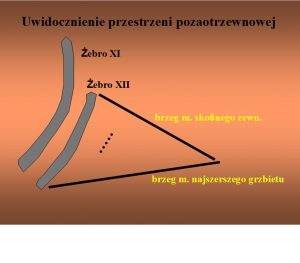
Formation of the retroperitoneal space


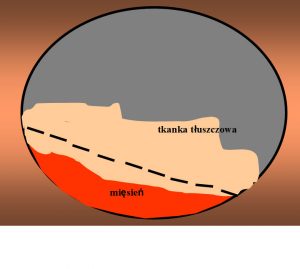
The procedure starts by making a 1 cm skin incision in the upper lumbar triangle. It is a triangle bounded by the 12th rib, anteriorly by the margin of the external oblique muscle and posteriorly by the margin of the latissimus dorsi muscle. The margins of the triangle are clearly marked, and the incision is made in the place of explicitly lower resistance.
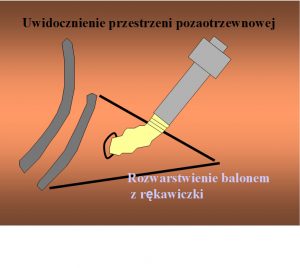
Then, using a blunt instrument, e.g. a paean, the layers are separated. After getting through the layers, in the same place the tissues are separated with the index finger placed into this space. In the next stage, a trocar with a balloon is inserted into the space thus prepared, and it is filled with 300-400mL of saline. The balloon is held for 5-10 minutes for distension and haemostasis, and then, after saline is drained, it is removed together with the trocar outside.

Then, a 10 mm trocar (optics) is inserted into the same place, through which carbon dioxide is administered to the retroperitoneal space to the level of 15 mmHg. Under visual control, 2 other trocars are inserted for the operator: in the mid-axillary line above the iliac crest and under the costal arch. Optionally, a fourth additional 5 mm trocar is inserted for the assistant and placed in the anterior axillary line.
PRZEBIEG ZABIEGU
Stage I – visualisation of the ureter
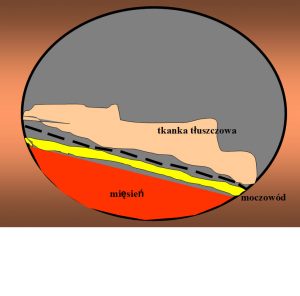
After introducing the optical system, the only point of reference in the retroperitoneal space is the iliopsoas muscle which must be made visible. Moving along the anterior margin of the muscle, the ureter is reached. Dissection of the ureter may cause certain problems, especially in obese patients.
Stage II – visualisation of the renal hilum
After dissection, the ureter can be caught with a grasper, clipped and severed.
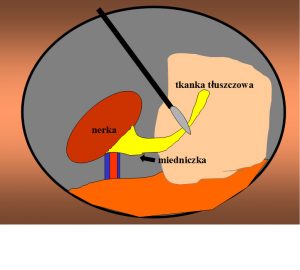
Moving along the ureter, the enal pelvis and the hilum are reached.
The tissues can be safely separated because in the retroperitoneal approach the renal artery is visualised as first.
Stage III – dissection and cutting renal vessels
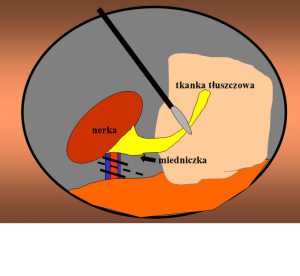
The artery is dissected first and easily clipped and cut. Then the vein is dissected, clipped and cut. Since small cirrhotic kidneys are generally removed by this approach, 11 mm clips are sufficient to occlude the vein. Optionally, the vein is closed with 12 mm endostapler.
Stage IV – cutting off the renal poles
After closing the vessels, the kidney is to be released from the surrounding tissues. Its inferior pole is visualised by pulling upwards the severed ureter. Then, moving along the dorsal part of the kidney, the peritoneum is shifted as fast as possible or, in the case of operating on a cirrhotic post-inflammatory kidney, it is cut off with scissors from the surrounding tissues. Because the patient is in the lateral position, the kidney is slightly going down and exposes its anterior surface. This stage of the procedure is not difficult. Releasing the superior pole is more complicated, especially when the kidney is located high.
If it is necessary to remove the adrenal gland, small vessels arising from the aorta, inferior vena cava and diaphragm should be dissected, clipped or coagulated. If the adrenal gland is not removed, it is cut off from the kidney using a dissector with bipolar coagulation or scissors with monopolar coagulation.
Stage V – extraction of the kidney outside
The kidney, together with the renal adipose capsule, is placed in a special bag. At this stage of the procedure, the surgical bed after the removed organ is inspected, haemostasis of small vessels is carried our and a drain is inserted. Then the organ placed in the bag is extracted. This can be done by making a small 4 cm-long incision, e.g. in the hypogastrium. We can also morcellate the kidney inside the bag using forceps or a morcellator, and then extract it outside through a 10 mm trocar. At the end of the procedure, the places remaining after the insertion of 10-12 mm trocars are dressed by suturing fascias and the skin. Only skin sutures are applied on places remaining after the insertion of 5 mm trocars.